Ed Giesbrecht & William C. Miller
University of British ColumbiaIntroduction
Performance of a skilled activity involves both motor and cognitive demands. Current theory suggests there is a finite capacity to meet these composite demands. If the activity requirements exceed resource capacity, performance will suffer, ostensibly at the expense of either motor or cognitive function. Divided-attention is the ability to manage competing motor and cognitive demands concurrently. Dual-task activities have typically been used to assess this capacity for divided attention.
Aging is associated with a decline in motor, sensory and cognitive function. Disability, stemming from such impairment, can result in greater demands for activity performance. For older adults, these demands may approach their total capacity and, particularly if additional attention demands are encountered, pose a risk to successful performance. These risks may include decreased proficiency in activity performance and potential injury from insufficient performance or lack of attention to environmental risks.
Mobility is the most common area of impairment among older adults, contributing to a high risk for falls and related injuries. Ambulation is a prime example of an essential activity that requires divided attention. At first blush, ambulation might appear to be an intuitive skill. Despite being well practiced, it requires considerable motor planning, multi-sensory process and response to environmental conditions. The Walking While Talking (WWT) test was devised as a quick and efficient assessment of divided attention and has proved fruitful in capturing information about mobility performance, and predicting future falls, frailty, disability and mortality among older adults (Verghese, Holtzer, Lipton & Wang, 2012). However, no comparable measure has been developed for older adults who use a wheelchair for mobility.
An estimated 1 million American older adults use a wheelchair for personal mobility. As with ambulation, learning and performing wheelchair mobility skills also demands considerable motor, sensory and cognitive processing. Not surprisingly, wheelchair tips, falls and related injuries are also common. One could presume that the same principles hold true for wheelchair mobility as in ambulation, that if the activity demands exceed personal capacity, performance with suffer – at the expense of either motor/sensory or cognitive/attention functions. Compromised performance could result in safety issues or inefficient propulsion, stemming from motor-sensory errors or insufficient attention to environmental obstacles.
purpose
We constructed a tool that would provide a measure of divided attention capacity for wheelchair mobility among older adults, comparable to the Walking While Talking test for ambulation. Such a tool could potentially offer insight into wheelchair users’ mobility skill proficiency in a competing context, simulating a real-life environment of divided-attention demands. Such an outcome could reflect skill integration/proficiency and safety/risk, as well as potential for learning more complex skills.
methods
Two conceptual models were incorporated into the design of this research project. Benson and Clark (1982) propose a 4-stage procedural template for developing measurement tools: Planning, Construction, Quantitative Evaluation and Validation. Switzer et al (1999) identify key issues to address when developing a modified/hybrid research instrument (i.e. converting the WWT test to the Wheeling While Talking test), which are synchronous with Benson and Clark’s design.
| RESEARCH STAGE & ELEMENTS | KEY ISSUES | STAKEHOLDERS |
|---|---|---|
| 1. PLANNING: | ||
| Purpose | Justification for Modified/Hybrid Tool | PI |
| Literature Review | Describe Original Tool & Inadequacies | PI |
| Initial Item Generation | Describe Selection of Test Items | Ad hoc Team |
| Validation by Expert/Stakeholders | Modifications to Original Tool | Research Group |
| Synthesis of Review/Feedback | PI | |
| 2. CONSTRUCTION: | ||
| Create Objectives | PI | |
| Items to Assess Objectives | Grad Students | |
| Appropriate Format | Grad Students | |
| Content Validation by Experts | Pool of Items based on Expert Feedback | Research Group |
| Administer to Sample for Feasibility | Pilot Testing | Grad Students |
| Revise for Use | Re-evaluate and Reduce if Necessary | PI |
| 3. QUANTITATIVE EVALUATION: | ||
| Pilot Test for Feasibility & Feedback | Collect Data | Grad Students |
| Reliability Estimates | Evaluate Reliability & Validity | Grad Students |
| Further Revision if Required | PI | |
| 4. VALIDATION | ||
| Multiple Research Efforts | PI | |
| Correlate with Other Measures | PI | |
| Hypothesis Testing | PI | |
An iterative process was used to develop and refine the WhWT test, employing four distinct stakeholder groups. Figure 1 illustrates the four stages, key issues and associated stakeholder groups. The principal investigators (PI) were involved in the conceptualization and literature review during the Planning stage; synthesizing data and feedback during the Construction stage; and overseeing data collection in the Quantitative Evaluation and Validation stages. An ad hoc team of work-study students, lead by a doctoral student researcher, engaged in the initial development of tool items during the Planning stage. An established group of wheelchair mobility researchers, composed of academic faculty, graduate students and post-doctoral investigators, provided input and critique at the Planning and Construction stages. Finally, a group of three occupational therapy graduate students, under the supervision of the first PI, developed the tool protocol, pilot tested (Construction stage), and measured reliability in the Quantitative Evaluation stage. The Discussion section that follows describes the process and outcome/results of each stage.
discussion
Literature related to the WWT test was reviewed to guide tool construction. Several variations of the WWT have been used in previous studies, so the most current and psychometrically evaluated version was chosen as a template. We established several criteria for the new measure to remain as true as possible to the constructs of the WWT. The motor task should require constant motor and sensory processing without being too complex, fatiguing or time-consuming to perform. Simply replicating the WWT task (i.e. walking 20 feet, turning, and walking back) was dismissed as individuals could potentially push their wheelchair and ‘coast’, rather than having to respond constantly to dynamic contextual demands as they would if ambulating. The cognitive task needed to be sufficiently challenging to demand attentional resources that could potentially impact or slow motor performance, but not be so difficult that individuals with diverse education or cognition could not easily understand the performance expectation.
During the planning stage, we generated several motor tasks (i.e., wheeling straight; around a distance obstacle; ‘slalom’ maneuvers around a variety of pylon configurations) and verbal/cognitive tasks (i.e., alphabet forwards, backwards and alternating letters; months of the year; spelling; counting backwards; etc.). The Ad Hoc Team, some with considerable wheelchair training and propulsion experience and some with none, trialed a wide variety of task combinations, assessing feasibility based on the criteria identified. A wheelchair research group was then presented with background related to the tool development and a summary of the Ad Hoc team’s findings. The merits and limitations were debated and critiqued, providing insight and direction for the PI to formulate items for inclusion in the tool.
We tasked a group of 3 graduate students in occupational therapy to refine the tool and create an administration protocol. The tool, at this point, was a 25 foot slalom course (50 feet total, there and back) with pylons aligned in 2 potential formats: 3 pylons roughly 8 feet apart with a 4 foot wide turnaround or 5 pylons 5 feet apart with a 3 foot turnaround. The verbal task required participants to recite alternating letters of the alphabet while propelling the obstacle course. Several scoring options were proposed: time to complete the motor task alone (baseline); time to complete the dual-task condition; time difference (dual-task – baseline); relative time difference (difference/baseline); number of obstacles hit during each condition; total number of letters recited; number of verbal errors (non-alternated letters) and error rate.
An informal pilot test was conducted using a convenience sample of 10 graduate students with a wide range of wheelchair use experience, blinded to the purpose and format of the test. Participants were sequestered and brought in one at a time to perform the baseline condition and then the dual-task conditions on the 5-pylon version test before moving to a separate room to repeat on the 3-pylon version test. Participants then completed a brief experiential questionnaire related to clarity of instruction, complexity of the tasks, safety and fatigue with performance.
Data from the pilot test is presented in Table 1. While the participants varied considerably in their experience and proficiency with wheelchair mobility, two students were sufficiently slow to be considered outliers; the table reflects scores inclusive and exclusive of these individuals’ data.
| Outliers | 5 Pylon Course |
3 Pylon Course |
||
|---|---|---|---|---|
| Included | Excluded | Included | Excluded | |
| Baseline (sec) | 31.6 | 27.5 | 21.6 | 18.5 |
| Pylon Hits | 0.6 | 0.7 | 0.0 | 0.0 |
| Dual-task (sec) | 36.4 | 32.1 | 24.9 | 20.4 |
| Pylon Hits | 1.1 | 1.0 | 0.1 | 0.1 |
| Difference (sec) | 4.8 | 4.7 | 3.3 | 1.9 |
| Percent slower | 16.8% | 18.9% | 13.6% | 10.7% |
| Total Letters | 19.5 | 16.6 | 14.8 | 12.8 |
| Errors | 1.7 | 1.5 | 0.3 | 0.3 |
| Error Rate | 8.0% | 8.4% | 1.8% | 1.7% |
Several trends emerged from the analysis. In the first (5 Pylon) trial, three participants were actually faster performing the dual-task condition, suggesting a learning effect for propelling and maneuvering the wheelchair (i.e., some participants lacked sufficient skill to accurately perform the task in the absence of any distraction). The lower rate of hitting pylons and making verbal errors in the second (3 Pylon) trial may support this conclusion. Some participants were noticeably challenged in trying to figure out how to effectively maneuver the wheelchair around the pylons without running over them. Others, being young, healthy and active individuals, seemed to be competitively motivated to complete the task quickly, despite instructions to “wheel at a normal pace”. By the second (3 Pylon) trial, these issues seem to have largely resolved. While the rate of slowing down for the dual-task condition was less with the 3 Pylon course, the variability in scores was substantially reduced (data not shown) and there were virtually no pylon hits, suggesting inexperienced participants had acquired a sufficient level of proficiency by this point. We concluded that most individuals who self-propel a wheelchair would have sufficient experience and skill to manage the demands of turning around an object on the floor and the frequency of hitting the obstacle would be low. Furthermore, there is no advantage to running over the pylon as this tends to slow the participant down. If the additional demands of the dual-task condition result in participants striking or running into a pylon, this would further confirm compromised performance capacity and potential for safety issues. On this basis, we chose not to include pylon hits in the scoring scheme, although it could be documented as additional information.
The verbal task required sufficient cognitive engagement to impact the motor task performance time, as reflected in both the raw and relative change scores. The number of letters recited was comparable between the 5- and 3-Pylon courses when adjusted for time to completion. However, the error rate was much lower in the 3-Pylon course. This may be reflective of a learning effect; however, the similar impact on the motor task performance (i.e., similar rates of slowing) suggests the cognitive demand is retained despite the higher degree of accuracy. To partially address a verbal task learning effect, we had participants practice starting with the letter “A” and then perform the test starting with “B”. In addition, participants begin at mid-alphabet in the 3-Pylon course (i.e. “M” and “N”).
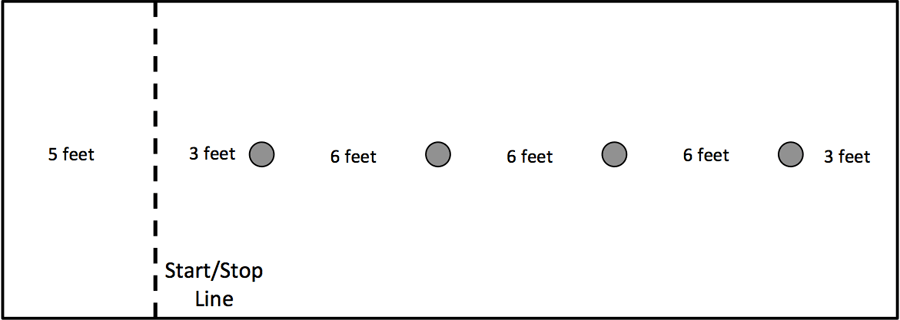 Figure 2. Layout of the 4 Pylon Course
Figure 2. Layout of the 4 Pylon Course Based on the pilot study findings, we made a number of adaptations to the test items. In consideration of the course layout, we chose to modify the course to a 4-Pylon format over the same distance (Figure 2). This provided a more equal distribution of left and right turns with a reasonable distance (6 feet) for negotiating the pylons. We incorporated an initial motor task demonstration, having the participant follow the administrator around the pylons to ensure they are familiar with the expectations and understand how to ‘weave’ through the course. After completing a timed baseline (motor task only) condition, the verbal task is explained and participants demonstrate a few letters, starting with “A”. Then a timed dual-task condition is administered, but starting with the letter “B”. A protocol manual and scoring sheet were created to standardize administration and scoring.
This beta-version of the test and manual were then presented to the Research Group to review and a practical session conducted with members. Feedback on the validity and feasibility was used to finalize the protocol manual.
As recommended in the literature, the next stages of tool development should be evaluation of reliability and validity. Under the direction of the first PI, the 3 graduate students involved in the tool development are currently conducting a study of test-retest, intra-rater and inter-rater reliability among older adult wheelchair users in a residential care setting. To address validity, the PIs are incorporating the Wheeling While Talking test as a tertiary outcome measure in a randomized control study investigating the impact of a wheelchair skills training program among community-dwelling older adults. This will enable exploration of any associations with measures of wheelchair skill capacity and safety, as well as personal factors.
conclusion
Measures of divided attention, such as the WWT test, have proved useful for estimating safety and functional proficiency among ambulatory older adults. Adapting the WWT for wheelchair use shows promise to offer similar benefits for a large and ever-growing demographic. This project systematically developed the Wheeling While Talking tool and is currently establishing the psychometric properties required to facilitate use in clinical and research settings.
References
Benson, J., & Clark, F. (1982). A guide for instrument development and validation. American Journal of Occupational Therapy, 36(12), 789-800.
Switzer, G., Wisniewski, S., Belle, S., Dew, M. & Schultz, R. (1999). Selecting, developing, and evaluating research instruments. Social Psychiatry and Psychiatric Epidemiology, 34, 399-409.
Verghese, J., Holtzer, R., Lipton R., & Wang, C. (2012). Mobility stress test approach to predicting frailty, disability, and mortality in high-functioning older adults. Journal of the American Geriatrics Society, 60, 1901-1905.
acknowledgements
The authors would like to acknowledge the numerous individuals who contributed to the project including our Ad Hoc testing team and our Wheelchair Research Group. In particular, we’d like to thank our 3 graduate student investigators Nicole Brinkman, Patricia Nordstrom, and Stephanie Runtz for their pilot testing and data collection work.